
As parents, we’re always concerned about the well-being of our children, especially when it comes to their physical development. One common concern that parents may have is toe walking, a condition in which a child walks on their toes instead of their whole foot. While this may seem harmless, it could be a sign of an underlying problem. In this article, we will discuss what toe walking is, its possible causes, when to take actions, how to treat it, and we’ll share some tips for parents.
TL;DR – the highlights:
- toe walking is a common condition in children where they walk on their toes instead of their whole foot
- it may be related to structural abnormalities such as tendon contracture or leg length discrepancy, or neurological/neuromuscular conditions such as autism, cerebral palsy or muscular dystrophy
- most cases of toe walking are idiopathic, with no discernable underlying cause
- an intervention may be necessary if toe walking persists beyond the age of 2-3 years or if it’s accompanied by other developmental problems
- treatment options include physical therapy, stretching exercises, orthotics, and in rare cases, surgery
What is toe walking?
Toe walking is a term used to describe a gait pattern in which a child walks on their toes or the ball of their feet, without putting their heels on the ground. It’s common in infants and toddlers who are learning to walk, but it usually resolves on its own as they grow and develop. However, if toe walking persists after the age of 2-3 years or becomes a habit, this may be a sign of an underlying condition.
In the normal version of toe walking, the child may walk on their toes but relax into a flat foot when standing still or on request. Normal adult heel-to-toe gait should prevail by age 3, but some children continue to walk on their toes. In children who develop toe walking after a period of walking on their heels and in those in whom toe walking is unilateral, the underlying pathological cause of toe walking should be considered.1
What are the possible causes of toe walking?
Although most toe walkers are otherwise healthy children, it’s important to approach each case with a high index of suspicion as toe walking may be a result of compensation for a short limb, or a manifestation of autism spectrum disorders (ASDs). Toe walking can be a symptom of certain neurological conditions, such as cerebral palsy or muscular dystrophy. Structural problems with the foot, such as a short Achilles tendon, can also cause toe walking.2
Here are the possible causes of toe walking in children, including:
- neurological conditions, such as cerebral palsy or muscular dystrophy
- muscle tightness or contractures
- developmental delays
- autism spectrum disorder
- genetic disorders
- structural abnormalities in the foot or ankle
But sometimes we can’t identified the underlying cause, in which case we’re talking about idiopathic toe walking.
What is idiopathic toe walking?
Idiopathic toe walking is a diagnosis given to healthy children who persist in walking on their toes after they should normally have achieved a heel-toe gait. The estimated prevalence of idiopathic toe walking is about 5% of healthy children3, and the condition affects boys more often than girls.4 It’s usually diagnosed when a child is over 2-3 years old and has been toe walking for an extended period of time.
Idiopathic toe walking is a diagnosis of exclusion; a diagnosis can only be made when other possible diagnoses have been ruled out.2 It’s a diagnosis made when a child normally walks on their toes, but no neurological, structural, or sensory cause is identified. It’s often diagnosed after a thorough evaluation by a physical therapist or other healthcare professional.
Although idiopathic toe walking doesn’t necessarily indicate an underlying problem, it’s still important to monitor your child’s development and seek medical advice if you have any concerns.
When should we intervene?
An intervention may be necessary if the child’s toe walking persists after the age of 2-3 years or if it’s accompanied by other developmental problems. It’s important to seek the advice of a healthcare professional if you have any concerns about your child’s development or if toe walking is causing pain or difficulty with activities (tripping, difficulty keeping up with peers).
If your child is a habitual toe walker, it’s important to have them evaluated by a physical therapist or other healthcare professional to determine the underlying cause. Depending on the cause, treatment may include stretching exercises, orthotics, or other interventions.
It’s also important to intervene if your child has pain or difficulty with activities due to toe walking. Prolonged toe walking can lead to shortening of the Achilles tendon and other muscle imbalances, which can lead to long-term problems if left untreated. For example, overuse of the calf muscles can cause muscle spasms that can lead to pain. Toe walkers may be prone to ankle sprains5 and have a less efficient gait, with reduced step length and increased cadence leading to increased energy expenditure.6
How do we treat toe walking in children?
Treatment for toe walking in children will depend on the underlying cause. In cases where no underlying cause can be identified, treatment may not be necessary. However, if there is an underlying problem, treatment options may include physical therapy, stretching exercises, serial casting, orthotics or in more severe cases, surgery.

Conservative methods are effective in most children with idiopathic toe walking, and conservative methods can be managed in primary care. However, if these methods are not successful, it’s appropriate to refer the child to a pediatric orthopedist for further evaluation.
Physical therapy
In physical therapy, we prevent compensatory forms of movement by encouraging correct movement patterns, symmetry in movement and posture, and we encourage proper loading of the feet and help the child learn to walk with the whole foot on the ground. If muscle weakness is contributing to toe walking, strengthening exercises may be recommended. These exercises can help improve the strength of the muscles that control dorsiflexion (lifting the foot toward the shin).
Stretching exercises for the plantar flexors
This can help lengthen the Achilles tendon and stretch the calf muscles that can be tight in habitual toe walkers to improve range of motion. A physical therapist can provide guidance on the appropriate stretches to do and how often to do them.
Manual passive dorsiflexion by a parent or therapist is often ineffective due to the plantar flexor strength seen in children. Therefore, we prefer stretching techniques that utilize the child’s body weight.7
Serial casting
Casting involves the application of short leg casts in maximal dorsiflexion for 4–6 weeks. In children with limited dorsiflexion, casts are changed every 1 to 2 weeks, with each cast change gaining additional dorsiflexion. Casting theoretically works by two mechanisms. Firstly, the child has no choice but to walk with heel contact while in the cast, which is full time, and this can break the ‘habit’ of toe walking. Secondly, casting provides a continuous stretch to the Achilles tendon.2
Serial casting should be accompanied with physical therapy to encourage proper movement patterns and proper loading of the feet. These casts are walkable, so they don’t affect the child’s strength, as temporary weakness usually doesn’t develop. However, they may have some difficulty with sensory feedback after the casts are removed as their feet may be a bit wobbly.

Orthotics
The rigid insoles, often made of carbon fiber8 theoretically work by providing sensory feedback or perhaps by limiting the flexibility of the foot, thereby making it difficult to toe walk. Ankle and foot orthosis (AFOs) with a plantar flexion block limit plantar flexion beyond neutral.
AFOs may be reasonable postoperatively for some children after surgical lengthening or after a serial casting to prolong the effect of casting, but in general are not the preference for first line treatment of idiopathic toe walking.2
In the case of limited range of motion, night AFOs for stretching may be a good option for prolonged stretch of shortened calf muscles.
Surgery
In rare cases, surgery may be required to correct structural abnormalities. Surgical lengthening of the Achilles tendon is an option in children with limited dorsiflexion. After surgical lengthening, a postoperative cast in a dorsiflexed position is usually required for 4–6 weeks to facilitate healing in a lengthened position. Depending on the type of lengthening performed, children may be allowed to bear weight in the casts. Operative complications may include excessive lengthening with associated weakness or painful scarring.2
Surgery is always the last option if nothing else is effective. But the first option is always conservative treatment, as we first try the other described treatment options.
It’s essential that parents understand that surgically lengthening or actually stretching the muscle will only resolve the contracture and allow the heel to touch the ground: the urge/desire to be a tip toe walker often remains as it’s centrally driven. The child must relearn the gait pattern to become a heel-to-toe walker.1
Suggested treatment plan
The optimal treatment for idiopathic toe walking has not been fully elucidated. It’s often helpful to reassure parents that toe walking doesn’t cause back pain, hip pain, or arthritis. The preferred primary treatment for children younger than 5 years, with dorsiflexion above neutral, is observation, as most toe walking resolves by this age.3 In children with dorsiflexion of the ankle greater than 10°, further observation is possible, and in children with very pronounced toe walking or with limited dorsiflexion of the ankle, a cast can be applied. Surgical lengthening is considered in children in whom the casting is unsuccessful or who have very limited range of motion and are unable to achieve dorsiflexion to a neutral position. For children who achieve good dorsiflexion but still have the “habit” of toe walking, an AFO may be considered.2
Advice for parents
Usually, the caregiver notices a gait abnormality compared to siblings or peers. Poor balance, frequent falls, pain, and fatigue are other possible concerns.
Encouraging the child to walk with a heel strike has not been shown to be effective9, which is probably due to the child’s short attention span. Children will often walk with a heel strike for a few steps and then return to walking on their toes. Verbal cueing to walk with a heel strike can be frustrating for both the child and the family.
What you can do is to choose a small section of the road (e.g., from one bench to another) to practice walking with a heel strike. And in the meantime, don’t talk, but try to let your kid focus on walking. When you reach the end of this ˝practice line˝ forget about it and let your child walk as usual. Walking is an automatic process, and we don’t have to think about how we walk, how we move our legs and arms, but if you want to change the walking pattern, you must really pay attention to, which is hard for kids to do consciously.
Here are some tips for parents who have a child who is toe walking:
- Talk to your child’s healthcare provider: If you notice your child is toe walking, it’s important to seek the advice of a healthcare professional. They can help determine if there is an underlying condition that needs to be addressed.
- Provide supportive footwear: Choose shoes with good support and a firm sole that can help encourage a heel-to-toe gait pattern.
- Perform stretching exercises: If your child’s physical therapist recommends stretching exercises, be sure to perform them regularly. Consistency is key when it comes to stretching.
- Stay positive: Encourage your child and focus on his progress, rather than his setbacks. It can take time to correct a toe walking habit, but with patience and persistence, it’s possible.
Brief instructions for performing stretching exercises for the plantar flexors
Stretching exercises can help lengthen the calf muscles and the Achilles tendon, which can be tight in habitual toe walkers.
Here are some instructions for performing a simple calf stretch:
- Stand facing a wall with your hands on the wall at shoulder height.
- Step back with one foot, keeping the heel on the floor.
- Bend your front knee and lean forward (with your hips, not your trunk), keeping your back leg straight and your heel on the floor.
- Hold the stretch for 15-30 seconds and then switch sides.
- Repeat the stretch 2-3 times on each leg, several times a day.
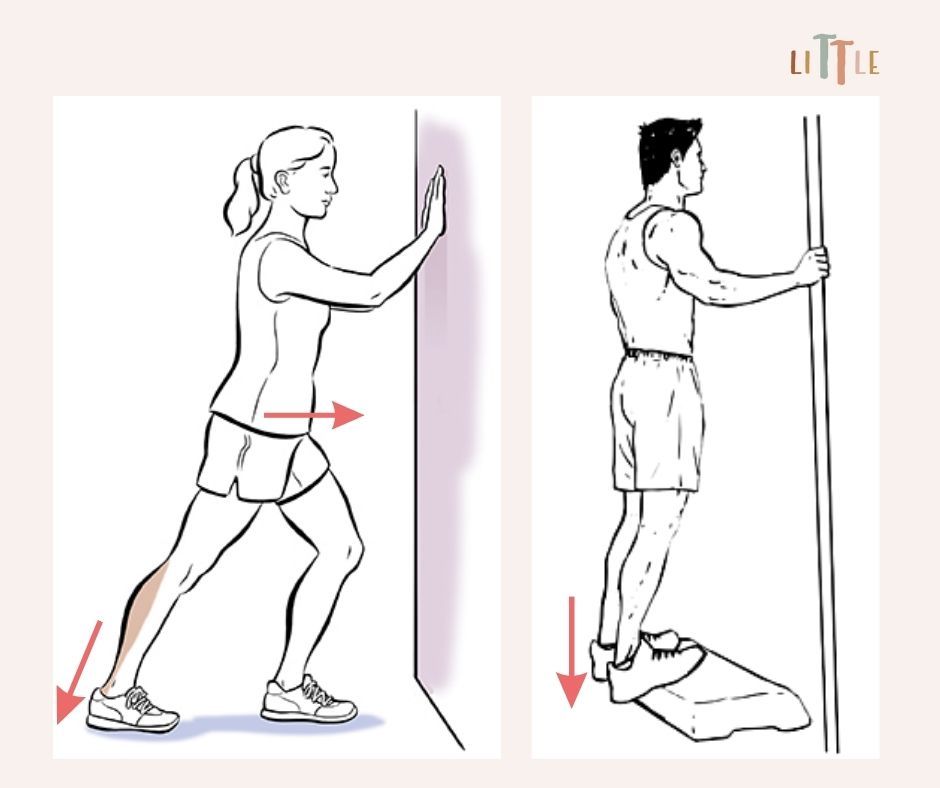
Alternatively, the child can stand with his feet on a board or step and then drop the heel down.
Toe walking can be a common occurrence in children, but it’s important to have it evaluated if it persists or becomes a habit. By working with a physical therapist and following their recommendations, most cases of toe walking can be successfully treated. Remember to stay positive and encourage your child along the way.
REFERENCES:
- Johnston, L., Eastwood, D. & Jacobs, B. (2014) Variations in normal gait development. Paediatrics and Child Health, 24(5), 204– 207. doi: https://doi.org/10.1016/j.paed.2014.03.006
- Ruzbarsky JJ, Scher D, Dodwell E. Toe walking: causes, epidemiology, assessment, and treatment. Curr Opin Pediatr. 2016 Feb;28(1):40-6. doi: 10.1097/MOP.0000000000000302
- Engström P, Tedroff K. The prevalence and course of idiopathic toe-walking in 5-year-old children. Pediatrics. 2012 Aug;130(2):279-84. doi: 10.1542/peds.2012-0225
- Engelbert R, Gorter JW, Uiterwaal C, van de Putte E, Helders P. Idiopathic toe-walking in children, adolescents and young adults: a matter of local or generalised stiffness? BMC Musculoskelet Disord. 2011 Mar 21;12:61. doi: 10.1186/1471-2474-12-61
- Goldstein M, Harper DC. Management of cerebral palsy: equinus gait. Dev Med Child Neurol. 2001 Aug;43(8):563-9. doi: 10.1111/j.1469-8749.2001.tb00762.x
- van den Hecke A, Malghem C, Renders A, Detrembleur C, Palumbo S, Lejeune TM. Mechanical work, energetic cost, and gait efficiency in children with cerebral palsy. J Pediatr Orthop. 2007 Sep;27(6):643-7. doi: 10.1097/BPO.0b013e318093f4c3
- Babb A, Carlson WO. Idiopathic toe-walking. S D Med. 2008 Feb;61(2):53, 55-7. PMID: 18432151.
- Herrin K, Geil M. A comparison of orthoses in the treatment of idiopathic toe walking: A randomized controlled trial. Prosthet Orthot Int. 2016 Apr;40(2):262-9. doi: 10.1177/0309364614564023
- Williams C, Tinley PD, Curtin M, Nielsen S. Foot and ankle characteristics of children with an idiopathic toe-walking gait. J Am Podiatr Med Assoc. 2013 Sep-Oct;103(5):374-9. doi: 10.7547/1030374
