
Flat feet is a common condition in children that can cause concern for parents. However, in most cases, it’s not a cause for alarm and will resolve on its own as the child grows and develops. It’s important to be aware of the signs that may indicate the need for medical intervention and seek the advice of a healthcare professional if necessary.
TL;DR – the highlights:
- flat feet are common in children and most children outgrow it
- obese and overweight children are more likely to have flat feet
- there is no evidence that a longitudinal arch in a child’s foot can be created by using orthotics or proper footwear, but this may reduce pain and improve alignment of the lower limbs
- the treatment is mainly aimed at the symptoms of pain and the severity of the deformity
- children must be physically active to fully exercise the muscles and ligaments of the foot arch
- walking barefoot can stimulate the correct development of the arch of the foot and thus prevent flat feet
What are flat feet?
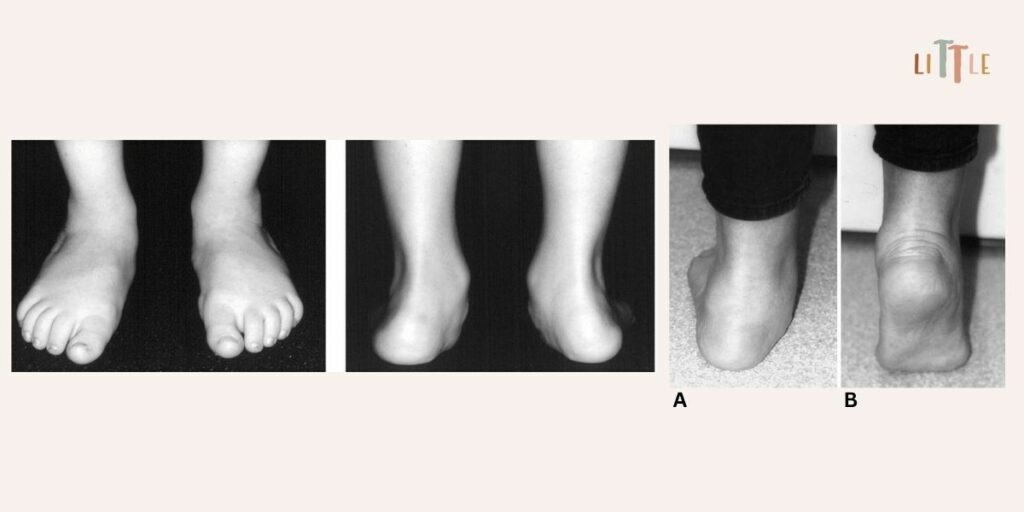
Flat feet, also known as pes planus, is a condition in which the arch of the foot is flattened, causing the entire sole of the foot to touch the ground. The condition is common in infants and young children, and usually resolves on its own as the child grows and develops.

Flat feet occur as part of normal development: infants are born with flat feet and have no detectable medial arch, which is covered by a fat pad until they start walking. As the child grows, plantar fat is resorbed, muscles develop and joint laxity decreases, leading to the formation of a medial arch.1 The medial arch usually appears between 2 and 3 years of age.2 Due to the physiological laxity of the ligaments, the lack of a medial arch usually persists throughout the years of toddlerhood and early childhood. Among children aged 3 to 6 years, 44% have flat feet.3 Physiological laxity of the ligaments usually improves with age and most children develop an arch in the first decade of life. However, flat feet tend to persist among overweight and obese children.
What subtypes of flat feet do we know?
There are two main subtypes of flat feet: flexible flat feet and rigid flat feet.
Flexible flat feet are the most common type and are part of normal development, usually present from birth. They are associated with joint laxity. The arch is visible when the child is non-weight bearing or standing on tiptoes but disappears when the child stands flat on his feet.2
Sometimes flexible flat feet are accompanied by a short Achilles tendon, in which case the condition is pathological. This occurs in older children and can account for 25% of flat feet in adults. The diagnosis is confirmed when less than 10 degrees of dorsiflexion can be achieved with the knee fully extended and hindfoot valgus corrected. Most patients improve with simple stretching exercises, although a few symptomatic patients may require surgical lengthening of the tight tendon.2
Rigid flat feet, on the other hand, occur when the foot arch is absent, both when the child is sitting and standing on the toes. Rigid flat feet are less common than flexible flat feet and can be a cause for concern as they may require medical intervention.2
What are the possible causes of flat feet?
Flat feet can be caused by a variety of factors, including genetics, developmental abnormalities, and muscle imbalances. Here are some possible causes:
- Genetics: Flat feet can be inherited from parents. If one or both parents have flat feet, their child may also be more likely to develop flat feet.
- Developmental abnormalities: Some children may be born with conditions such as cerebral palsy or Down syndrome, which can affect the development of the muscles and bones in their feet and lead to flat feet.
- Muscle imbalance: An imbalance or weakness in the muscles of the feet and legs can cause the arch to collapse and lead to flat feet. This weakness can be caused by a variety of factors, such as delayed motor development, tight or shortened muscles, or lack of physical activity. Low levels of physical activity could lead to delayed or uneven muscle strength, resulting in poor arch muscle strength.
Most flexible flat feet are physiologic, asymptomatic, and don’t require treatment, although other neurologic (cerebral palsy), muscular (muscular dystrophy), syndromic (trisomy 21), or connective tissue disorders (Marfan’s and Ehlers-Danlos syndrome) should be actively sought. Some cases of flexible flat feet can be painful, with more specific problems after activity.4
Who is more likely to develop flat feet?
Compared to girls, the rate of flat feet is higher in boys. This may be related to the fact that growth and development occur earlier in girls than in boys. Postural balance and physical development also occur earlier in girls. The physiological process of the growth of the foot arches from low to normal arches occurs earlier in girls, the development of the medial longitudinal arch in boys is slower than in girls, and the plantar fat pads in boys are thicker than in girls.5
Children who are overweight and obese are also more likely to have flat feet. Obesity significantly affects the structure of the feet in children. In addition, overweight children are more likely to have movement disorders and consequently avoid sports activities. Over time, this leads to weight gain and an increased incidence of flat feet.6
When should we intervene?
Children rarely have symptoms, with parental concern mainly related to cosmetic problems or the misconceived belief that the condition may cause pain or functional problems later in life. While most cases of flat feet in children are nothing to worry about, there are some signs that may indicate the need for medical intervention. Parents should pay attention to the following:
- pain or discomfort in the feet, ankles, or legs
- easy fatigue in the foot and ankle
- difficulty with higher level mobility tasks, such as running, jumping and hopping
- frequent tripping or falling
- noticeable difference in shoe wear
- difficulties with activities that require a long-standing position, such as sports or dancing.
If any of these signs are present, it’s important to seek medical attention from a physical therapist or other healthcare professional who can evaluate your child’s feet and recommend appropriate treatment. Treatment is mainly aimed at pain symptoms and the severity of the deformity.
Children without arch development by the age of 10 may have limited potential for natural resolution of their flat feet. Children with a family history of flat feet are more likely to have persistent flat feet as adults. The prevalence of flat feet in adults is 15–23%.7
How do we treat flat feet in children?
In most cases, flat feet in children don’t require treatment, as the condition will usually resolve on its own as the child grows and develops. However, if the child has pain or difficulty with activities, several treatment options are available:
- Exercises: Certain exercises can help strengthen the muscles in the feet and legs, which can help improve the arch and relieve pain. This can include lifting on the toes, walking on the outer edge of the foot, balance exercises such as standing on one leg.8
- Shoe inserts and orthotics: Can help provide additional foot support and improve alignment of the lower limbs, especially when flat feet are associated with knock-knees. Depending on the severity of the condition, a physical therapist or pediatrician can recommend an appropriate orthotic device for your child’s needs. However, it must be custom made to provide support in the right place.
- Footwear: Children don’t need shoes with arch support, but in case of pain, proper footwear can help provide support and stability to the feet. Shoes with good arch support and a firm sole can help relieve pain and improve alignment. For mild cases, good quality footwear may be sufficient; however, shoes generally provide more protection than correction.8
- Surgery: In rare cases, surgery may be needed to correct flat feet. This is usually only recommended if the child is in severe pain or if other treatment options have been ineffective.
NOTE: There is no evidence that any external force or devices such as shoe insoles or orthotics can create a longitudinal arch in a child’s foot.9 But custom-made insoles that support the foot in the right place can stimulate the development of the arch of the foot, so that the child, due to the “discomfort” caused by the support, strengthens the muscles of the arch of the foot, as he subconsciously tries to move away.
Advice for parents
If you suspect your child has flat feet, it’s important to seek the advice of a healthcare professional. A physical therapist or pediatrician can assess your child’s feet and recommend appropriate treatment if necessary. In the meantime, here are some tips to ease any pain or discomfort:
- encourage regular physical activity to strengthen the muscles of the feet and legs,
- make sure that your child wears properly fitted shoes,
- limit the time your child spends standing or walking on hard surfaces,
- encourage barefoot walking to promote proper arch development and thus prevent flat feet.
However, children must engage in appropriate physical activities. Adolescents who are not yet fully developed should avoid strenuous work (such as carrying loads) and sports (such as lifting weights). They could engage in high leg lifting, jumping activities (such as rope skipping, long jump, high jump, vertical jump, etc.), and climbing activities (such as climbing a ladder, using balance beams, rope climbing, pole climbing, etc.) to fully exercise the muscles and ligaments of the arch of the foot.5
Some examples of exercises:
- walking on toes
- walking on heels
- activities to improve dynamic arch, such as walking barefoot on different surfaces (soft sand is great for this)
- bending of the toes (e.g. picking up a tissue/small rocks/nuts with the toes)
- balance training (standing on one leg, on stable/soft surface, combined with different tasks – passing the ball, circling with the other leg… the possibilities are endless)
- jumping and climbing activities.
Exercise programs are more effective when they include games and activities that can be incorporated into a child’s day.
It’s important to remember that flat feet in children is a common and usually harmless condition. With proper treatment and care, most children will outgrow it and live an active, pain-free life.
REFERENCES:
- Jones S, Khandekar S, Tolessa E. Normal variants of the lower limbs in pediatric orthopedics. International Journal of Clinical Medicine. 2013;4(07):12. doi: 10.4236/ijcm.2013.47A2004
- Johnston, L., Eastwood, D. & Jacobs, B. (2014) Variations in normal gait development. Paediatrics and Child Health, 24(5), 204– 207. doi: https://doi.org/10.1016/j.paed.2014.03.006
- Volpon JB. Footprint analysis during the growth period. J Pediatr Orthop. 1994 Jan-Feb;14(1):83-5. doi: 10.1097/01241398-199401000-00017
- Yeo A, James K, Ramachandran M. Normal lower limb variants in children. BMJ. 2015 Jul 7;350:h3394. doi: 10.1136/bmj.h3394
- Xu L, Gu H, Zhang Y, Sun T, Yu J. Risk Factors of Flatfoot in Children: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022 Jul 6;19(14):8247. doi: 10.3390/ijerph19148247
- Taylor ED, Theim KR, Mirch MC, Ghorbani S, Tanofsky-Kraff M, Adler-Wailes DC, Brady S, Reynolds JC, Calis KA, Yanovski JA. Orthopedic complications of overweight in children and adolescents. Pediatrics. 2006 Jun;117(6):2167-74. doi: 10.1542/peds.2005-1832
- Hosalkar HS, Spiegel D, Davidson R. The foot and toes. In: Kliegman RM, Stanton BF, Schor NF, et al., editors. Nelson textbook of pediatrics, 19th ed. Philadelphia, USA: Elsevier Saunders; 2011. pp. 2335–2344.
- Turner C, Gardiner MD, Midgley A, Stefanis A. A guide to the management of paediatric pes planus. Aust J Gen Pract. 2020 May;49(5):245-249. doi: 10.31128/AJGP-09-19-5089
- Mosca VS. Flexible flatfoot in children and adolescents. J Child Orthop. 2010 Apr;4(2):107-21. doi: 10.1007/s11832-010-0239-9
