
My baby’s foot is not straight but curved inward, giving it a bean-shaped appearance. Is this normal? As a matter of fact, many infants and toddlers start life with twisted or bowed feet. In this case, it’s called metatarsus adductus and is a common condition of the foot in newborns in which the front part of the foot, known as the forefoot, is turned inward. It’s usually nothing to worry about, as most children outgrow it. But in rare cases monitoring and treatment may be necessary. Learn more about why this happens and what can help straighten the foot.
TL;DR – the highlights:
- metatarsus adductus is a common foot deformity in newborns
- it causes the front half of the child’s foot to turn inwards
- a common cause is the position of the baby’s feet in the womb
- most children don’t need treatment – the foot often straightens as the child grows
- if treatment is required, it may include stretching, casting, or surgery
What is metatarsus adductus?
Metatarsus adductus is one of the most common foot deformities in newborns, occurring in one to two cases per 1,000 births. Normally, the outer border of the foot is straight. In metatarsus adductus (also known as metatarsus varus), the outer border of the foot curves inward, giving it a C- or a bean-shaped appearance. It differs from other congenital deformities of the foot in that it’s exclusively a deformity of the front part of the foot.
In some cases, the dynamic deformity is seen only during the child’s gait, called “searching great toe.” The foot appears straight at rest, but the front of the foot curves inward with movement as a result of the action of the big toe muscles. But in other cases, in addition to walking and running, the front of the foot also turns inward when standing. This is called in-toeing and can cause the child to stumble more, but this is completely normal as the baby learns to walk and is part of typical development.
Synonyms: metatarsus adductus, metatarsus varus, metatarsus adductovarus, pes adductus, metatarsus supinatus, forefoot adductus, hooked forefoot
NOTE: Don’t confuse this with clubfoot – in this condition, the tight, short tendons cause the baby’s foot to turn inward so severely that the bottom (sole) of the foot faces up or sideways.
What causes it?
It’s not entirely clear why some children develop metatarsus adductus. However there are three possible causes.
First, the deformity may be caused by increased intrauterine pressure, which is supported by the increased incidence of metatarsus adductus in twin births. This might be due to compression in the uterus during the development of the fetus or lack of amniotic fluid. As the fetus grows, there may be less room for growth inside the uterus, so the feet or one foot (often the left) are compressed into a position that causes adduction of the forefoot.
Additionally, bone abnormalities and abnormal muscle attachments may also be causes, but there is not enough evidence to support these assumptions.
How severe is the deformity?
When evaluating the foot, we should assess flexibility. Deformity can be classified according to the flexibility in passive correction. This can be done by keeping the heel in a neutral position and abducting the front of the foot to at least a neutral position. Usually, the line bisecting the heel should cross the space between the second and third toes. In patients with metatarsus adductus, the line will be directed to the lateral border. The deformity is classified as mild if the line passes through the third toe. If the line passes through the space between third and fourth toes, it’s considered moderate, and if it passes through the fifth toe, it’s severe. However if passive correction cannot be performed, the deformity is rigid – a consultation with the child’s doctor may be necessary.

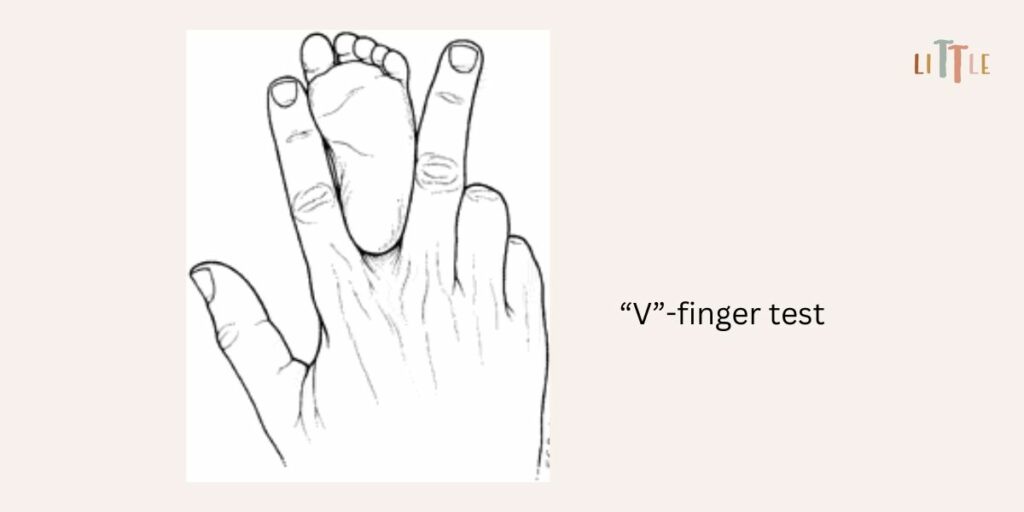
Here is a simple test you can do as a parent called the “V”-finger test. In this test, the heel of the baby’s foot is placed in a “V” formed by the index and middle fingers, and the lateral aspect of the foot is observed from a bottom side for medial or lateral deviation from the middle finger. A medial deviation from the middle finger indicates metatarsus adductus. This test can be used in cases where the heel is small enough to be placed in the space between the index and middle fingers.2
NOTE: Babies born with metatarsus adductus have a higher risk for developmental dysplasia of the hip, and further examination of the hip should be done.
When and how do we treat metatarsus adductus?
Most children who are born with metatarsus adductus do not need treatment. Up to 90% of cases resolve within 12 months.
Treatment is based on the severity of the condition. If the child has a mild or moderate deformity, it can be managed with stretching exercises during the first eight months of life. Flexible deformities lasting more than eight months or in cases of severe deformity that cannot be passively corrected may require serial casting.3 It’s prudent to wait until the child is over 6 months old before starting casting because many feet correct spontaneously.4 But we expect better results if treatment begins before eight months of age.5 Casts help stretch the soft tissues of the forefoot. The infant should have below-knee casts applied every 1–2 weeks for a period of 6–12 weeks to keep the foot in a straight position.6
Surgical treatment is only necessary in rare cases of rigid and severe deformities that do not respond to conservative treatment. Indications are usually residual metatarsus adductus in a child older than 3 to 4 years.4
On the other hand, there is no evidence that the use of foot orthoses, night time bars, shoe wedges or abduction shoes is effective in managing this disorder.7,8
What can I do as a parent?
- Gentle stretch
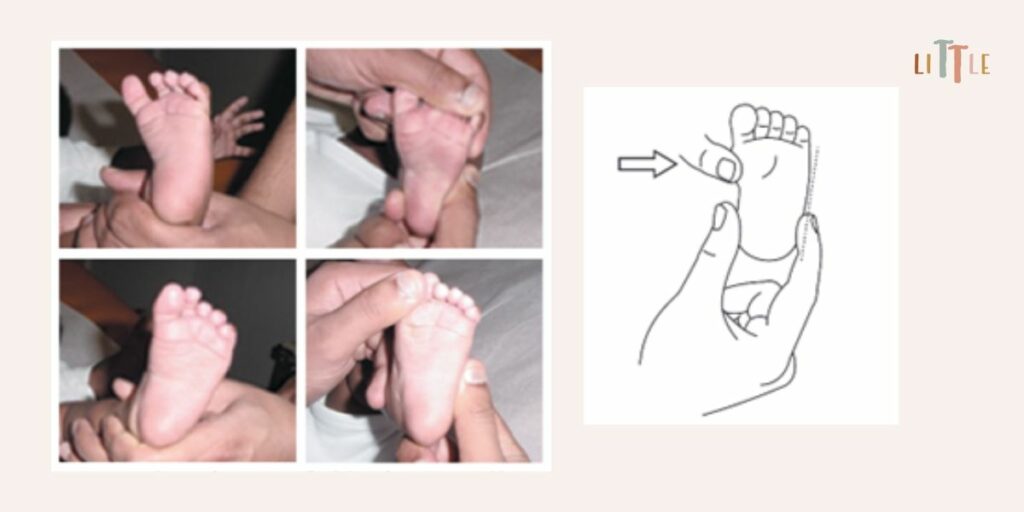
Grasp the child’s heel with one hand to fix it and gently pull the forefoot distally with the other hand and move the child’s forefoot outward so that it is straight – open the C-shaped curve and slightly correct it. You can hold this for a few seconds or longer if your baby is comfortable. We recommend that it’s done five times with each diaper change.9,10,11 However do not rotate or move the forefoot too much outward to avoid overstretching other structures of the foot.
- Muscle stimulation
Gently stroke the outside and front of your baby’s foot and lower leg to encourage the foot into a normal position. This may stimulate the muscles to work in the right direction, but it’s not based on evidence.
| Metatarsus adductus is common in newborns. However, consult your child’s doctor if: |
| • the feet are stiff and passive correction cannot be done |
| • the condition doesn’t improve with time. |
REFERENCES:
- Panski A, Goldman V, Simanovsky N, Lamdan M, Lamdan R. Universal neonatal foot orthotics-a novel treatment of infantile metatarsus adductus. Eur J Pediatr. 2021 Sep;180(9):2943-2949. doi: 10.1007/s00431-021-04048-5
- Connors JF, Wernick E, Lowy LJ, Falcone J, Volpe RG. Guidelines for evaluation and management of five common podopediatric conditions. J Am Podiatr Med Assoc. 1998 May;88(5):206-22. doi: 10.7547/87507315-88-5-206
- Williams CM, James AM, Tran T. Metatarsus adductus: development of a non-surgical treatment pathway. J Paediatr Child Health. 2013 Sep;49(9):E428-33. doi: 10.1111/jpc.12219
- Li YH, Leong JC. Intoeing gait in children. Hong Kong Med J. 1999 Dec;5(4):360-366. PMID: 10870163.
- Sass P, Hassan G. Lower extremity abnormalities in children. Am Fam Physician. 2003 Aug 1;68(3):461-8. Erratum in: Am Fam Physician. 2004 Mar 1;69(5):1049. PMID: 12924829.
- Katz K, David R, Soudry M. Below-knee plaster cast for the treatment of metatarsus adductus. J Pediatr Orthop. 1999 Jan-Feb;19(1):49-50. PMID: 9890286.
- Harris E. The intoeing child: etiology, prognosis, and current treatment options. Clin Podiatr Med Surg. 2013 Oct;30(4):531-65. doi: 10.1016/j.cpm.2013.07.002
- Uden H, Kumar S. Non-surgical management of a pediatric “intoed” gait pattern – a systematic review of the current best evidence. J Multidiscip Healthc. 2012;5:27-35. doi: 10.2147/JMDH.S28669
- Dietz FR. Intoeing–fact, fiction and opinion. Am Fam Physician. 1994 Nov 1;50(6):1249-59, 1262-4. PMID: 7942424.
- Churgay CA. Diagnosis and treatment of pediatric foot deformities. Am Fam Physician. 1993 Mar;47(4):883-9. PMID: 8438686.
- Bohne W. Metatarsus adductus. Bull N Y Acad Med. 1987 Nov;63(9):835-8. PMCID: PMC1629274
